A Convergence of Evidence:
Flower Essence Therapy in the Treatment
of Major Depression
An analysis by Dr. Jeffrey R. Cram
The convergence of findings from these five outcome studies strongly supports the concept that flower essences may be used adjunctively to facilitate the resolution of mild to moderate depression.
Abstract:
This article presents the findings of a series of studies conducted to determine the clinical efficacy of flower essences on the treatment of mild to moderate depression. Funding for the study was provided by the Flower Essence Society. Therapists participating in the study did so on a volunteer basis.
Five independent clinical outcome studies are presented, each lending evidence towards under-standing the clinical effects of flower essences on the treatment of depression. The results of these studies were measured using the Beck Depression Inventory (BDI) and the Hamilton Depression Scale (HAM-D). A time series analysis of the data was conducted using an ANOVA (analysis of variance) for repeated measures. Four of the studies were conducted by therapists in Cuba under the auspices of the Cuban Ministry of Public Health. The first of these studies examined over 100 patients, of which approximately half completed therapy. They were tracked over a period of five months, with an outcome indicating a significant reduction in depressive symptoms. The second and third studies utilized 20 patient/subjects and examined the effects of flower essence therapy over a 2-month and 3-month period of time. Again, significant drops in depression scores were noted during the first month, with further decreases during the second and third months. Both studies show reductions of the BDI total score of 76-77%. The fourth study utilized 24 cases over a 3-month period of time. Significant decreases in depressions were noted for the first two months, with this stabilizing at a 60 to 80% reduction during the third month.
The fifth study entailed a multi-site clinical trial conducted in the United States. It has been published elsewhere (Cram, 2001b). This study of 12 depressed subjects included a one-month baseline followed by 3 months of treatment that entailed usual care along with flower essence therapy. The findings indicated a stable baseline, followed by a 50% reduction in depression scores when flower essence therapy was introduced. This clinical change was maintained over a period of 3 months.
While none of these studies utilized a randomized control group, the convergence of findings from these five outcome studies strongly supports the concept that flower essences may be used adjunctively to facilitate the resolution of mild to moderate depression.
Depression and its Treatment
Once identified, depression can often be treated successfully with medication, psychotherapy, or a combination of both (Rush et al., 1993b). Not all patients respond to the same therapy, but a patient who fails to respond to the first treatment attempt-ed is highly likely to respond to a different treatment. Formal treatments for major depressive dis-order fall into six broad domains: medication, psychotherapy, the combination of medication and psychotherapy, electroconvulsive therapy (ECT), light therapy, and alternative therapies such as herbs and homeopathy. Each domain has benefits and risks, which must be weighed carefully in selecting the optimal treatment for a given patient.

Mariposa Lily is used to address disturbances in mother-child bonding.

Dr. Bach used Aspen as a remedy for unknown fears and anxiety.
The efficacy of the treatment of depression has been studied
extensively. Rush (1993b) conducted an exhaustive review of the
literature and presents the complexities of trying to monitor treatment
outcomes, along with “meta-analyses” of several forms of therapy. In one
such meta-analysis, 24 randomized control trials across 10 different
anti-depressant medications indicated that 57.8% of the patients
responded to anti-depressant medications, compared to 35.6% responding
to placebos.
Today, more and more individuals are seeking
non-pharmacological (alternative therapy) solutions to physical and
mental disorders. Eisenberg et al. (1993), conducted a national survey
indicating that one in three respondents used at least one alternative
therapy in the last year, and that a third of those saw their
alternative provider an average of 19 times. Similar international
studies estimate that from 70 to 90% of healthcare is rendered by
alternative practitioners (Micozzi, 1996). The nature of the studies
presented in this article focus-es upon the use of flower essence
therapy, one alternative therapy, in the treatment of mild to moderate
depression.
Flower Essence Therapy: Treating the Individual, Not the Disease
It is more important to know what sort of person has a disease than to know what sort of disease a person has. -Hippocrates
The practitioner considers the emotional, mental, physical, and spiritual aspects (or bodies) of the individual. There is not one standard flower essence or flower essence combination that is ideally suited for treating depression. Instead, the practitioner must treat the individual, rather than the disease, selecting the particular flower essence combination that will empower the individual to change. The essences are seen as catalysts for self-awareness and change. To be successful, rather than directly treating the depression, the essence combination for the individual must awaken the energetic qualities in the individual that are out of balance or suppressed.
Prior Clinical Research in Flower Essence Therapy
Flower Essence Therapy in Cuba
The emergence of flower essence therapy and the associated research in
Cuba is particularly significant. With the fall of the Soviet Union and
consequent ending of economic support, and the longstanding economic
embargo by the United States, by 1995, Cuba was faced with an unstable
economy, along with a scarcity of medical supplies and pharmaceuticals.
Because of the perceived efficacy and growing worldwide interest in
holistic medicine, the Cuban government mandated the establishment and
integration of natural and traditional medicine into their conventional
medicine national health system (MINSAP, 1996). Miyar (2002) has
provided a complete description of the revolution of political and
healthcare policy that led to educating healthcare practitioners in the
use of flower essences as the mainline treatment of mental and emotional
disorders. (See page 74 for an article by Dr. Miyar on flower essence
therapy in Cuba.) The systematic evaluation of the clinical effects of
flower essence therapy in the treatment of depression in Cuba was
stimulated by the previous research summarized in the preliminary
findings of Cram (2001b).
In this article, a series of clinical
outcome studies is presented that examine the clinical efficacy of
flower essence therapy as an adjunctive in the treatment of mild to
moderate severity in major depression. Four new, and one prior (Cram,
2001b), clinical outcome studies are presented in this article.

Holly was Dr. Bach's remedy for
healing the heart.

Milkweed can assist with overcoming emotional dependency.
A Time-Series Design Using the Beck and Hamilton Scales
In all of the studies, the impact of the flower essences on depression was measured on two objective standard depression inventories, the Beck Depression Inventory (BDI) and the Hamilton Depression Scale (HAM-D) (Beck, 1961; Hamilton, 1968). The former is a self assessment by the patient, while the latter is a structured clinical assessment by the therapist or physician.
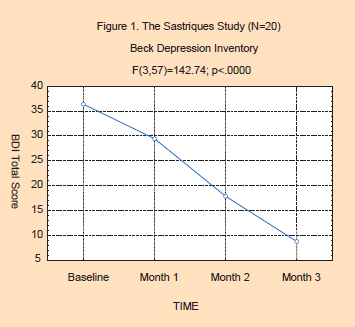
Study 1: The Sastriques Study: At the Outpatient Clinic of the Psychiatric Hospital of Havana
All 23 patients completed three months of flower essence therapy, most with four monthly Beck and Hamilton tests. The patients included 13 females and 10 males, ranging in age from 22 to 64, with an average age of 43. Of the 23 sub-jects, BDI and HAM-D data were complete for all four months for 20 subjects. There was an average of 5.2 essences selected in each session, and a total of 113 unique essences were used in the study. The twenty most frequently used essences were Agrimony, Scleranthus, Saguaro, Crab Apple, Olive, Oak, Borage, Mimulus, Impatiens, Holly, Gentian, Chestnut Bud, White Chestnut, Mountain Pride, Chicory, Rock Water, Self-Heal, Wild Rose, Aspen and Pomegranate.
The effects of flower essence therapy on both the Beck Depression Inventory (F(3,57)=142.74; p<.0000) and Hamilton Depression Scale (F(3,57)=175.07; p<.0000) were highly significant. Figures 1 & 2 show the significant declines in both the BDI and HAM-D scores. The BDI scores indicate that the group started out in the moderately depressed range at baseline, and ended in the “normal” range by the third month of flower essence therapy. The HAM-D scores reflect a moderate level of depression at baseline, shifting to mild levels of depression by the end of flower essence therapy.
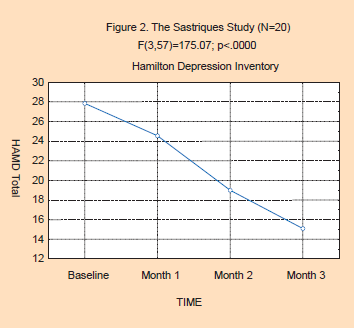
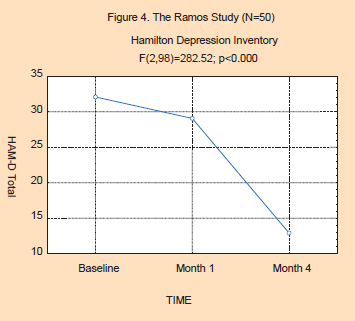
Study 2: The Ramos Study: An Active Practice of a Cuban Psychologist
One hundred and nine patients were offered flower essence therapy for their depression. Fifty-four patients, representing 49.5% of the sample, completed therapy, 19 patients were still under-going therapy at last report. Thirty-five patients abandoned therapy, and one patient died. The overall drop-out rate was 33%. The original sample consisted of 79 females and 30 males. The average age of the population was 47.4, ranging from 17 to 81 years. Patients were selected according to the criteria of the study: having had no previous flower essence therapy, reporting that they were depressed, and a willingness to volunteer for the study. Of the 54 completing the study, Hamilton Depression Scores were completed less often, with baseline and first month data available on all subjects with only 50 HAM-D assessments being conducted at the 5th month of therapy.
Individual prescribing procedures were utilized, based on a clinical interview with the patient. The 54 patients were seen monthly over the course of their therapy, for a total of 5 visits. An average of 3.2 flower essences were used in each session, out of a total of 98 unique essences. The twenty most frequently used essences were Mariposa Lily, Dandelion, Beech, Sunflower, Lavender, Garlic, Holly, Manzanita, Chamomile, Self-Heal, Chicory, Saint John’s Wort, Snapdragon, Angelica, Crab Apple, Saguaro, Yerba Santa, Forget-Me-Not, Willow, and California Wild Rose.
The results of the Ramos study are presented in Figures 3 and 4 below. As can be seen in the BDI scores, there is a highly significant change in BDI scores (F(4,148)=83.54; p<0.000). Here, the base-line for the depressed patients began in the high end of the severely depressed range, falling nearly 50% and into the bottom end of the moderately depressed range at the end of 4 months of flower essence therapy. Post hoc analysis, (Tukey’s HSD, Tukey, 1992) shows a significant decrease in depression scores for each month compared to the prior month. The HAM-D ratings by the prescribing physician also show severe levels of depression at baseline, with a highly significant decrease in depression (F(2,98)=282.52; p<0.000) being observed over the course of the 4 months. Here, there is a 66% decrease in the HAM-D scores from severely depressed at baseline to mildly depressed at month 4. Post hoc analysis (Tukey’s HSD) showed significant drops for each time period.
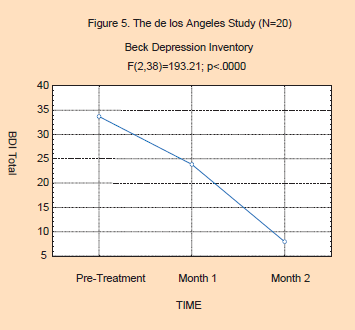
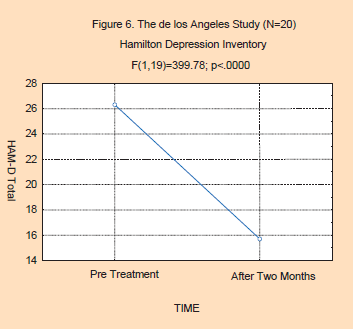
Study 3: The de los Ángeles Study: A Psychiatric Practice in Havana
Patients were selected according to similar criteria as in the Ramos study. The selected patients had no previous flower essence therapy, reporting that they were depressed, and volunteering to be in the study.
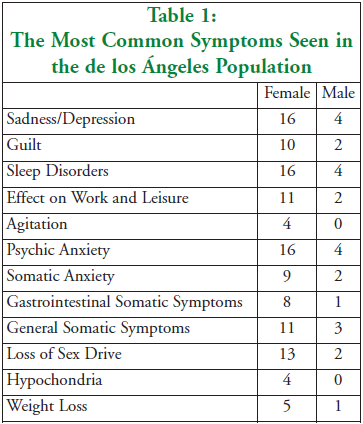
Twenty patients were studied. All patients who entered the study completed the two-month study; there were no dropouts. The mean age of the sample was 50.12 years, ranging from 21 to 80 years. There were 4 males and 16 females. Seven of the patients had been suffering from depression for less than 1 year, with the shortest duration of depression being 3 months. The rest of the population had been suffering from depression for more than 1 year. Two had a 2-year history of depression, two had a 3-year history of depression, three had a 5-year history of depression, and one had a 6-year history of depression. Seven of the patients were concurrently on antidepressants, 9 were also utilizing tranquilizers, and 5 were concurrently receiving psychotherapy. Table 1 shows the most frequent symptoms seen in this population.
As with the prior studies, individualized prescribing was done, while
using the EEI kinesiology method described previously to select flower
essences for each patient. The most commonly used essences for this
population were: Mustard, Gentian, Wild Rose, Borage, Bleeding Heart,
Star of Bethlehem, Sweet Chestnut, Honey-suckle, Gorse, Walnut, Chicory,
Pine, Agrimony, White Chestnut, California Wild Rose, Yerba Santa, Aloe
Vera, Milkweed, Sagebrush, Chamomile, Larch, Olive, Hornbeam, and
Love-Lies-Bleeding.
The results of this study are best
represented in the two figures below. As can be seen in Figure 5, the
BDI scores dropped significantly (F(2,38)=193.21; p<.0000) from
baseline through therapy. They began in the severely depressed range,
reaching the normal range by month 2. Post hoc analysis (Tukey’s HSD)
shows significant changes for each month. In Figure 6, we see a
significant decrease in HAM-D scores (F(1,19)=399.78; p<.0000). Here,
we see a 57% decrease in depression ratings, going from the moderately
depressed, down into the mildly depressed range.
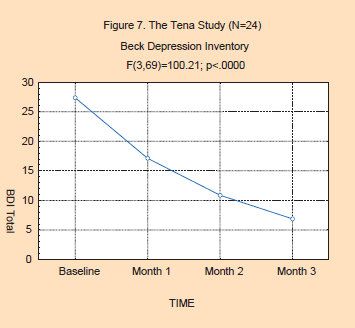
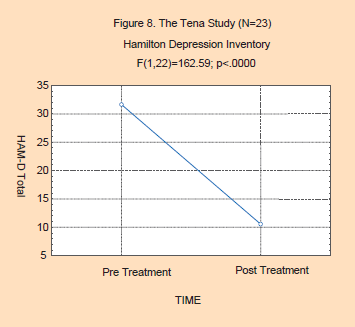
Study 4: The Tena Study: A Holistic Psychiatric Practice
Dr. Tena works solely with natural and tradition-al medicines, including flower essences, homeopathy, and acupuncture at the 26 de Julio Polyclinic, Playa Township, Havana. She has participated in various conferences in Psychiatry, Homeopathy, and Natural and Traditional Medicine.
She presented a paper on her depression study research at the Ninth
International Congress of Flower Essence Therapists (IX Congreso
Internacional de Terapeutas Florales) in Cuernavaca, Mexico, October,
2002. Portions of this article are based on data presented at that
congress.
Dr. Tena’s study provides a more complete picture of
the treatment outcome effects than the other studies, and contains much
descriptive data on the population studied.
Patients for the
study either showed up at the clinic on their own initiative for
treatment for depression, or, more frequently, were referred by other
doctors from the clinic where Dr. Tena works. Individual prescribing
procedures were utilized, based on a clinical interview with the
patient. Three of these subjects dropped out of the study, and there was
incomplete data on one subject’s initial HAM-D score, leaving 24
subjects for analysis for the BDI data and 23 subjects for the HAM-D
data. There were 21 females and 3 males. The mean age of the population
was 54.1 years, ranging from 33 to 75 years of age. The characteristics
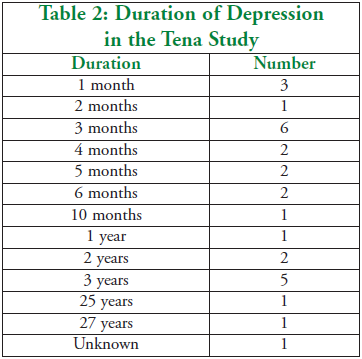
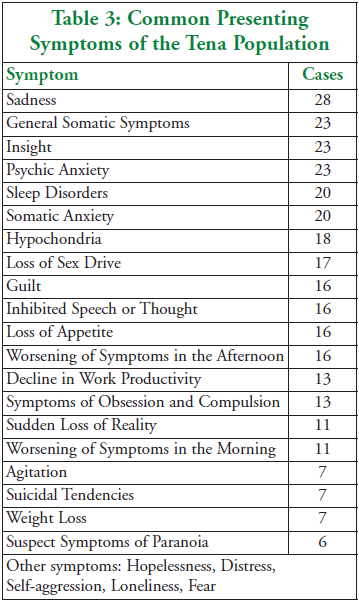
of depression are detailed in the tables on the next page. Table 2 shows
the duration of the depression, while Table 3 shows the major symptoms
of the group.

Chamomile relaxes emotional tension, especially in children.

California Poppy helps the soul gather its forces of light and warmth.
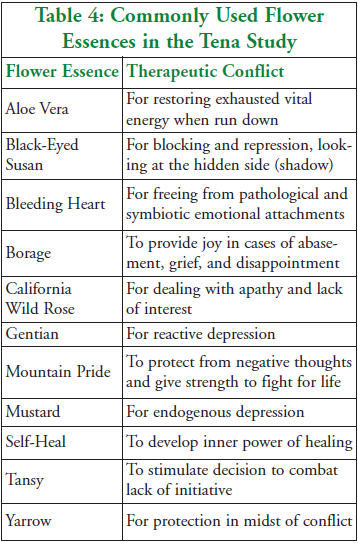
A total of 65 different flower essences were used for the 28 subjects. Table 4 shows the most commonly used essences and the therapeutic conflicts they address.
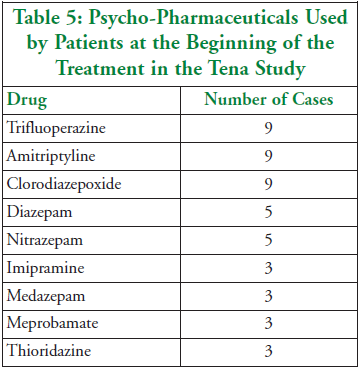
At the beginning of the
study, 26 of the 28 patients were taking psycho-pharmaceutical
medication. Dosages were gradually reduced and eliminated by the end of
the study. Table 5 shows the drugs that were used by patients at the
beginning of the study.
The outcome results of the study are
presented in the two figures below. As can be seen in Figure 7, there is
a significant decrease in the Beck Depression Inventory scores across
time (F(3,69)=100.21; p<.0000). Here, the levels of depression go
from the moderate range to the normal range. In addition, the effects of
the flower essences on depression tend to stabilize by the second month
of treatment. The data for the second and third months do not
significantly differ, while all other comparisons are significant using
Tukey's HSD. In addition, Figure 8 shows significant effects of flower
essences on the Hamilton Depression Scale as well (F(1,22)=162.59;
p<0000). The changes go from the severe range of depression to
“nearly normal” levels of mood and affect.
Study 5: The Cram Study: A Multi-Site Study in the USA
There were 12 subjects in this study, coming from four clinical trial sites. The sites are listed at the bottom of Table 7. Three of the clinical trial sites were psychotherapy practices, contributing 11 of the 12 subjects to the study. Two of the psychotherapy practices were transpersonal in nature, while the third was cognitive and behavioral in its approach. The non-psychotherapy clinic was a naturopathic practice in which a combination of nutritional support was offered along with wellness counseling. There were 3 male and 9 female subjects, aged 35 to 79 years of age, with a mean of 48.5 years. They had been depressed for an average of 22 years. Nine had tried antidepressants, while 3 had not. At the time of the study, 8 patients were currently on an antidepressant, and had been on these for an average of 17 months.
Treatment was comprised of usual care, followed by usual care in combination with flower essence therapy. In all but one clinical trial site, the usual care entailed psychotherapy. One clinical trial site utilized naturopathic counseling for usual care. Over the course of the experimental treatment phase, patients were offered an average of eight different flower essences. Across the 12 subjects, a total of 65 different flower essences were used. For any given patient, the range of essences used went from a minimum of five essences for 1 patient to a maximum of 13 different essences for another patient. The flower essence therapy utilized an “individualized” approach and was direct-ed by the philosophy of “treating the individual, rather than the disease (depression).” The particular flower essence combination used with a patient was selected based upon the areas in the patient’s life for which the therapist felt the patient needed support or were emerging as part of the counseling.
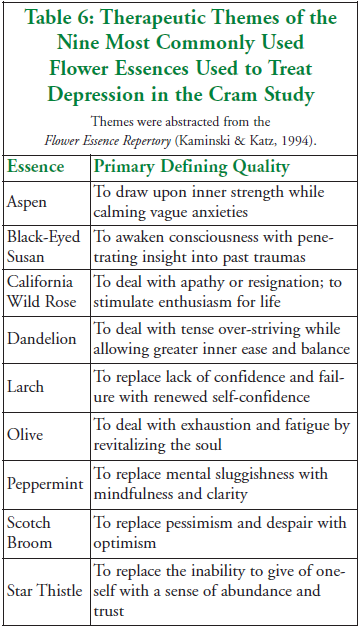
To give a sense of how flower essences are used clinically to treat depressed individuals in this study, the nine most common flower essences offered to these patients, along with their therapeutic themes, are listed in Table 6 (in alphabetical order). These essences occurred consistently in at least 25% of the patients.
The
results of the Cram study are presented at two levels. The first
represents simple descriptive statistics on the level of change in
depression for each subject, and the second analysis utilizes
inferential statistics.
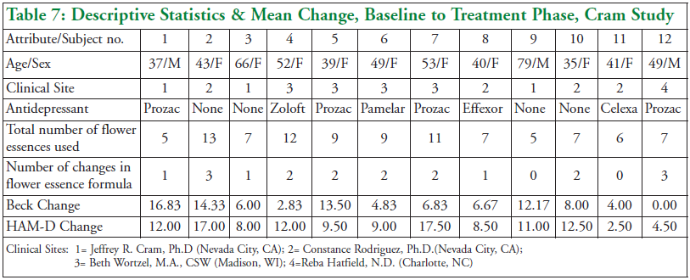
The descriptive statistics are presented
in Table 7 below. Along with the demographic of the subject, the
presence or absence of antidepressant use is described. In addition, the
total number of flower essences taken by the subject over the treatment
period is given, along with the number of times the clinician changed
the flower essence formula over the course of the patient’s care.
As
can be seen in this table, one half of the subjects made substantial
changes in their depression scores (Beck change scores that were 10
points or more), one third of the subjects made moderate gains, and only
2 subjects made minimal changes. One should note that there are some
discrepancies between the subjects’ self-ratings of depression (Beck)
and those of the therapists (HAM-D). The level of change in the
depression scores, however, does not appear to consistently sort along
the lines of the clinical site (therapist), the use of antidepressant
drugs, the total number of flower essences used to treat the patient, or
the number of times the therapist changed the flower essence formula
over the course of therapy.
In addition to the descriptive statistics above, two separate analyses using inferential statistics (ANOVA) were conducted. Each analysis involved an analysis of variance with repeated measures because of related samples. The first analysis considered the Period Effect. Here, the “within variable” had 5 levels (2 baseline, plus the 3 treatment measures.) In the second analysis, the interaction effects of concurrent use of antidepressants was considered. This was conducted using a group-blocking variable for current use of an antidepressant. As can be seen in Table 7, there were 8 subjects that were currently on antidepressants and 4 that were not.
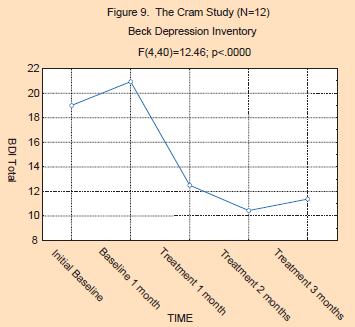
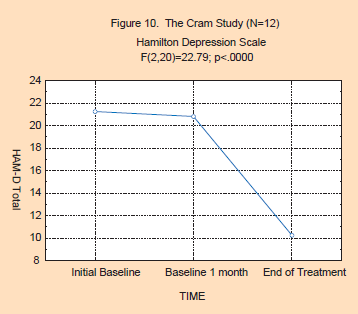
The
results for Period Effect are reflected in Figures 9 and 10. As can be
seen, the statistics on both the Beck Depression Inventory
(F(4,40)=12.46; p<.0000) and Hamilton scores (F(2,20)=22.79;
p<.0000) are highly significant, indicating that this Period Effect
is highly consistent. The post hoc analysis shows that the two baseline
data points are not significantly different from each other, while the
treatment data points for both the BDI and HAM-D were significantly
lower than the baseline points. Overall, the depression ratings dropped
by approximately 50% during the treatment phase for both the BDI and
HAM-D variables. These ratings shifted from the moderately depressed
range down into the lower end of the mildly depressed range.
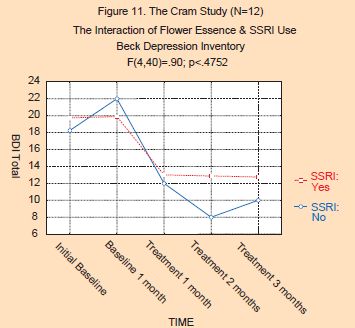
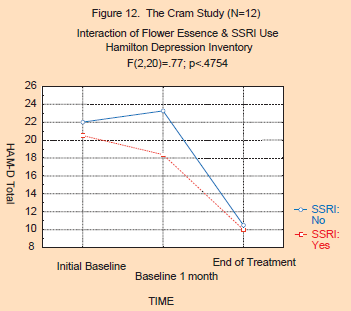
The
second analysis concerning the concurrent use of antidepressant
medications (“SSRI”) is presented in Figures 11 and 12. As can be seen,
the level of significance for the two-way interactions (Period x
Medication Group) was not significant for either the BDI (F(4,40)=.90;
p<.4752) or the HAM-D (F(2,20)=.77; p<.4754). The decrease in both
the BDI and HAM-D scores was similar, whether or not the subject was on
an SSRI. This suggests that the use of anti-depressants did not
interact with the effects of the flower essences, and strongly suggests
that the effect on depression was solely due to the flower essences, and
not the allopathic medications.
Discussion: Individualized Treatment
What is being tested in these studies is not a specific flower essence (or a specific combination of essences), but rather a method of individualized flower essence treatment.
It should be noted that there are several challenges to both the internal and external validity of these current studies. The first challenge has to do with “individualized” treatment versus standardized treatment. The “individualized” prescribing method of the flower essence practitioner certainly confuses the traditional operational definition of the independent variable. In the above studies, over 100 different flower essences were utilized, with an average of eight different essences being administered to a given subject. What is being tested in these studies is not a specific flower essence (or a specific combination of essences), but rather a method of individualized flower essence treatment. Such an “individualized” approach of “treating the individual, rather than the disease,” is very common in homeopathy. A recent meta-analysis by Cucherat et al. (2000) examined 118 clinical trials that involved individualized homeopathic therapies, and a slightly earlier meta-analysis by Linde and Melchart (1998) examined 32 clinical trials that compared individualized homeopathic therapies to placebo controls. While such an individualized prescribing approach does lend “noise” to the independent variable and the scientific method, it is the clinical method of choice for the alternative practitioner who uses flower essences, and thus should be allowed as a valid method.
Considering the Placebo Effect
However, in previous unpublished research on the use of flower essences on the treatment of depression, the senior author has conducted a pilot study on 6 subjects that employed a randomized double-blind placebo control group design. In this study, all 3 of the experimental subjects (flower essence) responded in the same fashion as did the subjects in the current study, with large, 50% or more, decrements in their BDI scores. In addition, 2 of the 3 placebo subjects (brandy carrier only) showed an impressive 50% decrement in BDI scores during the first month of treatment. However, by the second month of treatment, the BDI scores of the placebo responders were back to baseline and stayed elevated into the third month of placebo treatment. One of the placebo subjects was converted into a single case study format, and at the beginning of month 4, she was given the authentic individualized flower essence therapy. By the end of month 4, her BDI scores were reduced by 50% again. This time the BDI stayed down for the next 2 months. Such a crossover single subject design is very attractive, and lends evidence to the effectiveness of flower essences in the treatment of depression. Unfortunately, it is difficult to generalize beyond this one subject. It was the lack of generalization associated with single-subject designs that was the primary reason for the selection of the time series/within subject design used in the above studies.

California Wild Rose helps to bring enthusiasm into one's life.

Black-Eyed Susan shines light into the psychological shadow.
The problem with the placebo effect is not the fact that it exists. We
should all celebrate its existence. The problem with the placebo effect
is that its effects are typically short-lived and small in nature.
Recent evidence suggests that patients with different types of
depression and prognoses react differently to placebo and treatment.
Schatzberg and Rothschild (in press) reported that the placebo response
rate for non-psychotic major depressive disorder is on the order of 25%,
while the placebo response rate for psychotic depressions is only about
10%. The outcomes of the current study were in the 50% range, and far
exceed those solely attributable to the placebo response.
Next,
consider the duration of the placebo effect. Its therapeutic effects are
typically short-lived, lasting 2 to 4 weeks. In the Cram and Tena
studies, the 3-month treatment period is one of the strongest arguments
in favor of the fact that flower essences were more active than the
placebo effect. This is reflected in the fact that the changes in the
BDI and HAM-D scores endured over a 3-month period of time.
Some
might argue that depression typically resolves more slowly than over a
period of 4 months, and that that is why most studies of depression span
a period of 6 to 9 months. The 2-to 4-month nature of the current
studies may not allow one to examine the true nature of the treatment
response. Some patients, for example, may relapse after the initial
reprieve, while others may not respond to the treatment until the fifth
or sixth month. The 4-month duration of the current study lacks
follow-up and the possible assessment of relapse. Thus, the short
duration of these studies may possibly weaken their findings.
The fact that we see such significant response curves to the use of flower essences in all five studies clearly suggests that practitioners can use non-toxic, energetic substances to assist their patients in coping more effectively with depression.
A
secondary analysis of the data by Cram was conducted to determine
whether SSRI medications would interfere with the therapeutic use of
flower essences, and vice versa. This post hoc analysis did not show a
separation between the two groups (SSRI medicated and unmedicated) in
their responses to the introduction of flower essence therapy. Thus, it
appears that being on an SSRI does not interfere with the
psychotherapeutic and flower essence aspects of the treatment. One
should note, however, that the small number of patients in the medicated
and unmedicated groups, coupled with their self-selection, weakens our
ability to generalize the results to the population in general.
The
fact that we see such significant response curves to the use of flower
essences in all five studies clearly suggests that practitioners can use
non-toxic, energetic substances to assist their patients in coping more
effectively with depression. In a psychotherapy practice, flower
essences appear to pro-vide the practitioner with a tool to assist the
patient in resolving psychological issues that pertain to and perpetuate
depression. Some practitioners might think of a flower essence remedy
as a “transitional object” (Winnicott, 1953). For example, during the
psychotherapy session, the therapist might be assisting the patient to
become more aware of how the patient’s traumatic childhood plays a role
in her chronic depression. As part of the therapy, the practitioner adds
Black-Eyed Susan to the flower essence combination and tells the
patient that this will assist her in retrieving or resolving those
child-hood memories. The theme, initiated during the therapeutic
session, is facilitated and continued at home by the patient through her
use of the essence. The flower essences reinvigorate the theme as they
are taken orally on a daily basis.
The large number of
replications presented in this paper document the clinical effectiveness
of flower essences in the treatment of depression and provide a strong
and compelling basis for using these tools clinically to treat
depression. Further inquiry is, of course, needed. Randomized control
group studies would provide additional evidence, along with longer, 6-
to 8-month periods of treatment. Ultimately, randomized
placebo-controlled studies would provide the strongest base of evidence
as to the effectiveness of these nontoxic flower essences in the
treatment of depression.
Dr. Jeffrey Cram
Dr. Jeffrey Cram was the director of the Sierra Health Institute of Nevada City, California until his death in 2005. There he coordinated and treated patients using a holistic approach to psychology. This included such approaches as transpersonal psychology, cognitive behavioral therapies, biofeedback, flower essence therapy, aromatherapy, bioenergetics and music therapy. He was the founding president of the Surface EMG Society of North America (SESNA). He was the author of three books and 35 articles on surface Electro-myography, had an active interest in research, and was the Principal Investigator on several clinical studies. He was on the editorial list of four journals (AJPM, JAPB, JMPT, IJHC). Dr. Cram was an international expert on surface Electromyography and the use of flower essences in a psychotherapeutic practice.

To install this Web App in your iPhone/iPad press ![]() and then Add to Home Screen.
and then Add to Home Screen.
